ECR 2013 / C-1746
Pancreaticoportal fistula — A rare complication of pancreatitis
Congress:
ECR 2013
Poster Number:
C-1746
Type:
Educational Exhibit
Keywords:
Pancreas, Abdomen, Vascular, CT, MR, Fluoroscopy, Cholangiography, Fistula, Acute, Inflammation
Authors:
D. BARUAH1, P. P. Tolat1, J. Sullivan1, K. Christians 1, M. Laguna2; 1Milwaukee, Wi/US, 2Franklin, WI/US
DOI:
10.1594/ecr2013/C-1746
, prominence of the pancreatic duct (red arrow), and a calculus within the pancreatic duct (blue arrow). Note patency of the superior mesenteric vein (green arrow).")
Fig. 1:
Patient 1. Contrast enhanced axial CT images from 4/2008 demonstrate changes of...
 extending to the splenic vein and superior mesenteric vein (white arrow). Note the communication between the pancreatic head pseudocyst containing the calculus (green arrow) with the splenic vein (yellow arrow).")
Fig. 2:
Patient 1. Contrast enhanced axial CT images from 9/2009 demonstrate new fluid...
.")
Fig. 3:
Patient 1. T2 weighted axial MR image from 9/2009 shows the pancreatic...
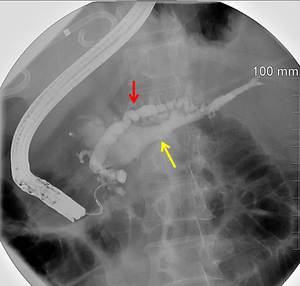
, and opacification of the portal venous system (yellow arrow denotes opacification of the splenic vein). Note also the pigtail catheter draining the large pancreatic pseudocyst.")
Fig. 4:
Patient 1. Single ERCP image from 3/2010 illustrates changes of chronic...

Fig. 5:
Patient 1. Contrast enhanced axial cine CT images from 4/2010 showing...
 and the persistent calculus within the superior mesenteric vein (yellow arrow).")
Fig. 6:
Patient 1. Contrast enhanced axial CT images from 10/2011 demonstrate the...

Fig. 7:
Patient 2. Contrast enhanced axial CT image from 12/2007 demonstrates acute...
. There is a communication between the pseudocyst and the portal vein (red arrow) as well as the pseudocyst and the splenic vein (yellow arrow).")
Fig. 8:
Patient 2. Contrast enhanced axial CT images from 12/2010 demonstrate a...
 and the portal venous confluence/ splenic vein (yellow arrow).")
Fig. 9:
Patient 2. Single coronal T2 weighted MRCP image from 12/2010 again illustrates...

Fig. 10:
Patient 2. Contrast enhanced axial CT images from 2/2011 showing similar...
 Axial and B) coronal CT images from 12/2010 demonstrate changes of acute pancreatitis with peripancreatic inflammatory stranding. C) Axial and D) coronal CT images from 10/2011 show persistent acute pancreatitis changes with pseudocyst formation (red arrow). The pancreatitc duct is also dilated (yellow arrow).")
Fig. 11:
Patient 3. Contrast enhanced CT images in a single patient with acute...
. There is new hypodensity within the expanded portal venous system (white arrow), which is contiguous with one of the pseudocysts (yellow arrow).")
Fig. 12:
Patient 3. Contrast enhanced axial and coronal CT images from 5/2012...
 Single image from 8/2005 shows findings of acute pancreatitis with peripancreatic inflammatory changes. B) Single image from 10/2008 illustrates a pancreatic head pseudocyst (red arrow). C-D) Images from 5/2012 show an enlarging pancreatic head pseudocyst and other changes of chronic pancreatitis, including pancreatic ductal dilatation and parenchymal calcifications.")
Fig. 13:
Patient 4. Serial contrast enhanced axial CT images demonstrate pancreatic and...
. There is hypodense content within the portal venous system (white arrow). The pseudocyst also communicates with the pancreatic duct (yellow arrow). There is cavernous transformation of the portal vein (green arrow). Incidentally noted are bilateral renal solid and cystic lesions.")
Fig. 14:
Patient 4. Contrast enhanced axial and coronal CT images from 11/2012...